|
This post, written by Kate Wiebe, originally was published on January 23, 2017, on the ICTG blog. How is your congregation generating goodness in the world today? A lot of people in the world, and particularly in the United States, feel distraught. They worry about having a job, having a home or shelter, getting a good education, having health care, and being safe – let alone being happy, feeling free, or having wealth to share. We witnessed this weekend how millions of people voted for the current administration and how millions of people marched against the current administration. Interestingly, many congregations today have members from both of these groups. They are struggling to bring reconciliation within their own walls, as well as in their communities. Loving a neighbor as yourself is a primary commandment. Perhaps what's most striking about the command to love one's neighbor is how it requires crossing so many arbitrary human-made lines . . . lines of faith, economic status, ethnicity, politics, and education. Learning how to love the person most different from you – to provide for them – stretches our capacities greatly. How is your congregation doing that now, in light of so much division? What's working best for you? When these things are developed, crises, trauma, and disasters are far less likely to occur. When they do occur, groups practicing these things are far more resilient.  As a Christian pastor, I also see how the story of the Good Samaritan inherently is about responding to trauma as well. Being a good neighbor means responding to the wounds my neighbor has with effective care. This weekend, as a country, we were presented with a lot of wounds in front of us. People who voted for the current administration, who have long felt forgotten and ignored. People who voted against the current administration, who have long felt forgotten and ignored and now fear it even more. And people who feel a wide range of other experiences, much of which is based on pain from the past. There are many people hurting. Many who have been hurting for a long time. The State of the Union is beleaguered, at best, and there is a tremendous amount of work to be done to stabilize it. Hope in joining together with people of like-mindedness. Hope in hearing a neighbor's story and thinking about their perspective in new light. Hope in deciding to fight for the rights and benefits of a neighbor, more than just one's own. Story after story keeps emerging across the country of a people who seek out liberty and justice for all. And, through all the pain expressed this weekend, millions of people witnessed glimmers of hope. Hope in joining together with people of like-mindedness. Hope in hearing a neighbor's story and thinking about their perspective in new light. Hope in deciding to fight for the rights and benefits of a neighbor, more than just one's own. Story after story keeps emerging across the country of a people who seek out liberty and justice for all. What is your congregation doing to participate in building up your community and the nation? It what ways are you making a difference for greater health and well-being? At ICTG, we’ve found, in part, the work of health and well-being gets done most often through individual or small group efforts that add up to great collective movements. They include:
When these things are developed, crises, trauma, and disasters are far less likely to occur. When they do occur, groups practicing these things are far more resilient. In the days ahead, may we all work toward building more healthy, vibrant communities. We all know the world could use a lot more them.
0 Comments
The following is an adapted excerpt from our training materials, which provide useful information for leaders to learn how to respond well to trauma.
VIEW TRAINING MANUALS
What Are Panic Attacks?
Panic attacks (abrupt periods of intense anxiety, fear, discomfort) can occur at any age and any stage of life. They occur when a person’s body temporarily is overloaded with stressful communication. Faith leaders may experience them, personally, in the aftermath of trauma, or may encounter them among people to whom they are ministering. Panic attacks usually last for 1-10 minutes, though some have been known to last for a few hours. Panic attacks can be scary. At the same time, they are common responses to trauma and usually are not life-threatening. Persons suffering from a panic attack often report feeling as though they are having a heart attack, “going crazy,” having a “melt down,” etc. Panic attacks are linked to “fight or flight” biological responses to threats, and they involve spontaneous flooding of the body with adrenalin and cortisol hormones. They are momentary chemical imbalances in persons’ bodies, which usually are attributed to external stresses or anticipatory anxiety and fear. What Can Contribute to Panic Attacks? However, a range of substances are known to overload a body’s communication and limit responsiveness when combined with heightened stressful environments. These substances include:
Keeping these in mind when you personally are under duress, or are working with individuals experiencing great stressors, may save you value time and energy in response. Any of these substances, or intense temperature changes, can initiate an internal biological shift. When combined with emotional strain and excessively stressful environments, they can overload bodily systems and induce panic attacks. Frequently, practicing methods of self-regulation and calming can help a person’s body begin to communicate well within itself and bring about overall senses of well-being.
Tips for Responding to Panic Attacks
When someone is having a panic attack, it's important to regulating the body as soon as possible. For example, you may have a person sit in a comfortable seat, in a mild climate, either indoors or outdoors. You may have them sip a cool glass of water, and steady her or his breathing. Use a gentle voice, reminding the person you are with them. Speak to them about how safe they are, here and now. You might ask them if they can feel physical things around them – the sturdiness of the ground and their seat. You may ask them to tell you what their throat, stomach, hands, or feet feel like. If any of these feel clenched, you may ask them if they feel they can relax them. Frequently, practicing methods of self-regulation and calming can help a person’s body begin to communicate well within itself and bring about overall senses of well-being. If calming is not possible, further medical or psychological professional assistance may be necessary. Share your Best Practices What's worked well in your community for caring for people suffering from panic attacks? Have you encountered these experiences? What's been most helpful? Share in the comments below.
Help sustain online education by making a financial contribution today or becoming a monthly donor. Thank you for your generosity!

This post, written by Kate Wiebe, originally was published on November 10, 2015, on the ICTG blog.
ACEs stands for the Adverse Childhood Experience Study. If you've been following this blog, you know we talk about them frequently. To learn more about them, you might try visiting the list resources below that explain why ACEs matter to communities and how medical professionals are beginning to address the massive problem. You also can find out more about the ACE study origins, as well as learn about an ever-expanding network of professionals who utilize this study in their own settings.

Perhaps most profound thing about the ACE study – besides the significant fact that it demonstrated trauma does not discriminate and exists in every community in the country – is the strong correlation it demonstrated between childhood experiences and adult onset illnesses.
The ACE study found that survivors of childhood trauma are nearly 5000% (yes, you read all those zeros correctly) more likely to attempt suicide, have eating disorders, or become IV drug users. Dr. Vincent Felitti, the study's founder and co-conductor, along with the Centers for Disease Control and Prevention, details this remarkable and powerful connection. "With an ACE score of six – experiencing any six of the ten categories that we studied – that person was 4,600% more likely to become an IV drug user than a person who experienced none of those six categories. Now you read in the newspaper the latest cancer cure of the week – prostate cancer or breast cancer increases 30% and everyone goes nuts – I'm talking 4,600% increase. The same ACE score of six produces a likelihood of attempting suicide between 3,100% and 5,000% greater than the likelihood of suicide attempts in someone with none of those life experiences. So the power of this relationship is enormous."
The magnitude of this correlation, and the complexity of dealing with the problem of severe stress in childhood after the fact is so huge, Dr. Felitti, says, realistically the only serious and effective approach is going to have to involve primary prevention. He admits, "No one knows how to do that, but it's the right question to focus on."
The only serious and effective approach is going to have to involve primary prevention.
At ICTG, we recognize how community groups, schools, after-school programs, and congregations are prime locations for not only putting that question at the forefront but also for providing primary prevention.
Trauma Informed Community Practices for Prevention
Ideally, our community's organizations are safe havens from life's storms. They are the place where play, education, worship, and mission derive from true restoration of body, mind, and spirit in community. Every day, you, as a leader or volunteer, are invited into making it so. Share your stories in the comments below about how you see healing from ACEs happening in your congregation.
Recommended Resources:
TED TALK by Nadine Burke Harris ACE STUDY ORIGINS by the CDC Center for Youth Wellness website ACES TOO HIGH website VIDEO by Vincent Felitti
Help sustain online education by making a financial contribution today or becoming a monthly donor. Thank you for your generosity!
This post, written by Kate Wiebe, originally was published on July 23, 2017, on the ICTG blog.
How do life experiences in childhood end up with disease states half a century later?
More community and faith-based leaders need to be engaging this question. For example, if you're a church or ministry leader reading this post, are you familiar with the ACE Study? Do you know how many of your members or visitors have experienced ACEs and what kind of ACEs they've experienced? How are those experienced impacting your mission? Put another way, to what extent does your mission interface with ACEs? How does your congregation or ministry group actively counter the effects of ACEs?
Have I lost you? If so, please allow me to explain. Your health, your organization's health, and the health of your greater community depend on your understanding ACEs and their far-reaching impacts. ACEs stands for Adverse Childhood Experiences. If you've been following this blog, you know we talk about them frequently. If you're new to the topic, learn more about them in the following ways:
Perhaps most profound about the ACE study – besides the significant fact that it demonstrated trauma does not discriminate and exists in every community in the country – is the strong correlation it demonstrated between childhood experiences and adult onset illnesses. The ACE study found that survivors of childhood trauma are nearly 5000% (yes, you read all those zeros correctly) more likely to attempt suicide, have eating disorders, or become IV drug users. In the video below, Dr. Vincent Felitti, the study's founder and co-conductor, along with the Centers for Disease Control and Prevention, details this remarkable and powerful connection. "With an ACE score of six – experiencing any six of the ten categories that were studied – that person was 4,600% more likely to become an IV drug user than a person who experienced none of those six categories. Now you read in the newspaper the latest cancer cure of the week – prostate cancer or breast cancer increases 30% and everyone goes nuts – I'm talking 4,600% increase. The same ACE score of six produces a likelihood of attempting suicide between 3,100% and 5,000% greater than the likelihood of suicide attempts in someone with none of those life experiences. So the power of this relationship is enormous." - Dr. Vincent Felitti The magnitude of this correlation, and the complexity of dealing with the problem of severe stress in childhood after the fact is so huge, Dr. Felitti, says, realistically the only serious and effective approach is going to have to involve primary prevention. He admits, "No one knows how to do that, but it's the right question to focus on." At ICTG, we recognize how many community-based and faith-based organizations are prime locations for not only putting that question at the forefront but also for providing primary prevention. At ICTG, given the evidence, we recommend organizational leaders consider to what extent their agencies, youth members, or volunteers have experienced ACEs. For faith-based leaders, we provide assessment tools to discern ACEs within your group and to gauge your organization's resiliency and response capacities in our General and Youth Ministry Resource Guides. Also, while becoming a trauma-informed congregation by creating a culture marked by specific traits, trauma-informed congregations can incorporate preventative measures into their common practices. Trauma Informed Practices for Prevention
Ideally, schools, after-school groups, and congregations are safe havens – healing sanctuaries – from life's storms. They are the place where learning, play, worship, confession, prayer and mission derive from true restoration of body, mind, and spirit in community. Every day, you are invited into making it so. Share your stories in the comments below about how you see healing from ACEs happening in your community. Find further education for leaders by browsing our services and training materials.
To support this blog and other educational and care services, give a financial gift today.
Individuals can experience trauma in a variety of ways, but their recovery will be improved when supported by a trauma-informed community. The hallmark characteristics of a trauma-informed community will be similar regardless of its type, which may include a school, a neighborhood group, a circle of friends, or any other supportive organization. Leading traumatologists like Bessel van der Kolk, Babette Rothschild, Robert Macy, Charles Figley, Don Catherall, Robert Anda, and Vincent Felitti have identified a number of aspects they’ve seen across trauma-informed communities.  What are the key traits of a trauma-informed community?
As communities seek to cultivate these trauma-informed practices, they express a sense of living in the world that directly counters trauma by acknowledging the truth of what has happened and creating a safe space to heal. *These traits are adapted for from a template provided by St. Aemilian-Lakeside, Inc., for providing trauma-informed care and based on the works of Bessel van der Kolk, Babette Rothschild, Robert Macy, Charles Figley, Don Catherall, Robert Anda, and Vincett Felitti. Interested in learning more trauma-informed best practices? Visit the ICTG TRAINING MANUALS PAGE or the SERVICES MENU to purchase ICTG’s most popular resource guides, assessments, modules, seminars, and more.
This post, written by Rev. Dr. Kate Wiebe, originally was published October 17, 2019, on the ICTG blog as an updated version of The Riviera Care blog post from August 21, 2019. Are you, members of your household, your neighbors, or your staff prepared for potential Public Safety Power Shutoffs (PSPS), led by power utilities, Southern California Edison and PG&E? Both utility companies have developed plans to shut down power during critical fire weather in order to reduce the risk of wildfires. It is important to know that the PSPS could lead to multi-day power outages in many areas all over California during periods of extremely hot, dry and/or windy weather.  How long is a PSPS outage expected to last? The utility companies say that a PSPS outage will last as long as the potentially dangerous weather conditions exist, plus the amount of time it takes for their workers to inspect and repair their equipment in any affected area(s). They recommend that residents be prepared to endure a power outage lasting 3-5 days. Are you prepared for a power outage lasting 3-5 days, or more? Power outages impact the whole community and can make it difficult for people to meet their basic needs, as well as:
How else can you prepare?
Further Resources To Learn More About PSPS from Power Companies, contact:
Additional Preparedness Resources for California:
For better organizational preparation consider contacting ICTG for further services, referencing our resource guides, and reading more of our blogs. 
The Institute originally published this post on June 18, 2013, on the ICTG Blog.
What happens when a community, a group, an organization, or a family is hurt? Social Relations theorists suggest that a group responds in similar patterns as a body or a person. Today, many of our community and faith-based bodies are hurting. Although it is not new to human experience, with the help of social media and mass media, we are more acutely aware of the long-term mental, emotional, and spiritual toll that traumatic events take. We see more clearly that disaster-torn towns and cities cannot be restored simply with hammers and nails.
For years, though, especially in North America, hammers and nails were the very definition of Long-Term Recovery. If you were engaged in Long-Term Recovery efforts, then you likely sat on a committee or volunteered with a short-term mission group or donated business assets in efforts to fix facility needs. For years, long-term mental, emotional, or spiritual needs were relegated to professional services, and salved by routine care practices that were singular and for the most part disconnected from one another beyond basic referrals. These practices may meet individual, family, or small group needs. Yet, when community-wide events occur, disaster relief experts are finding that efforts must be more coordinated across public services. Otherwise, towns and cities end up exhausting themselves by duplicating efforts, mis-communicating, and overlooking unmet mental, emotional, and spiritual care needs.

Best practices do exist and are emerging for more effective and efficient community-wide care. Law enforcement, emergency management, and therapeutic and social work agencies are making use of trauma-informed education. City and county VOAD (VOLUNTARY ORGANIZATIONS ACTIVE IN DISASTER) groups are coordinating multi-profession communication. Faith leaders are becoming informed, actively involved in, or are leading community-care initiatives. As these kinds of care practices continue to take shape and gain momentum, communities will be skilled in responding to mass trauma events in ways that promote healing and growth.
Sustain free online education by making a contribution today. Your generosity makes a great difference!
This post originally was published on September 11, 2018, on the ICTG blog.
These days it can feel as though there are few places to turn where you do not encounter the impacts of trauma in some form. Whether you are marking the 17th anniversary of 9/11 today or the one-year anniversaries of hurricanes Irma, Harvey, and Maria, or you are preparing for the incoming storms of Florence or Olivia, you are in the thick of your own crises related to flooding, violence, fire, substance abuse, depression, anxiety, death, or terminal illness – it can be hard not to feel overwhelmed and even hopeless amid the chaos of heartache.
Trauma, of course, is not new. Though it may be decades or even centuries since events like the ones we face today have occurred, the sustainable practices of resiliency remain the same across time and demographics. Here are some of the ways leading field experts, journalists, and scholars are naming them today: Pediatrician and leading Adverse Childhood Experiences (ACEs) scholar, Dr. Nadine Burke-Harris on the prescription plan for countering adversity:
Collective traumatologist,Dr. Jack Saul, on the four themes most typical of a functional community resilience and recovery approach:
Pastoral theologian, Dr. John Swinton, on the relational and spiritual practices for formation through and beyond loss:
These practices are not merely about being "good" or "healthy." They are proven to be the skills and practices that sustain individuals, families, and groups through widely ranging forms of loss. To learn more about how you or your organization can practice skills for resiliency, browse ICTG's downloadable guides, training materials, or contact us to learn more.
Help sustain online education by making a financial contribution today or becoming a monthly donor. Thank you for your generosity!
This post, written by Rev. Dr. Kate Wiebe, originally was published June 17, 2019, on the ICTG blog. Almost two years ago now, board director emeritus and former clinical psychologist, Rev. Dr. Gordon Hess, PhD, wrote on this blog. It's about how ICTG started out five years ahead of the curve on topics of trauma, groups, and communities. It may be hard to believe, especially these days when it can seem like nearly everyone is talking about trauma, PTSD, brain science, fight/flight reactions, and long-term impacts of adversity, but back when ICTG was starting in 2012 it felt like hardly anyone was talking about these critical issues. We reviewed the original ACEs study and considered how those statistics may be reflected in schools, congregations, and businesses. Then we compared that with the types of disasters that had occurred around the country during the early 2000s. We saw an immense need to inform organizational leaders and provide coaching and therapeutic services for them. Our tremendous donors, volunteers, and staff have been doing that ever since. 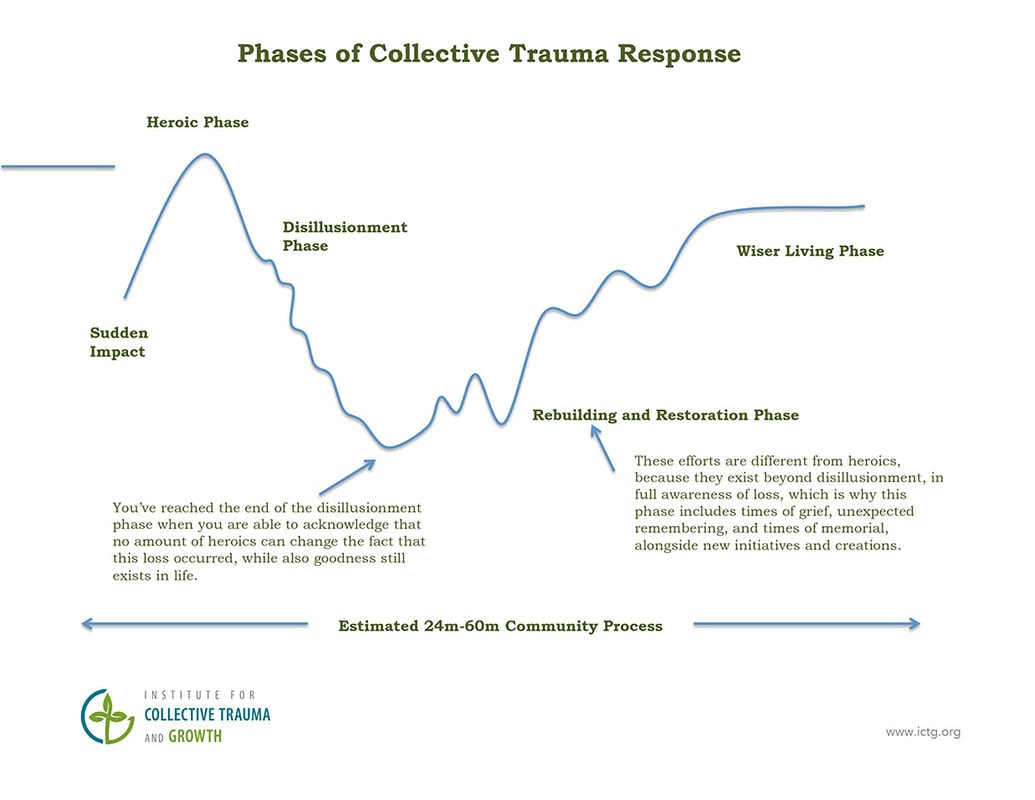 Though we're immensely grateful to see more resources becoming available to organizational leaders, we see that many resources, like the Phases of Disaster Response, and the current categories for disaster funding (which segment according to the type of incident that has occurred, such as a tornado or a wildfire or an act of terror), do not fit the mold of challenges communities are facing today. This great disparity further complicates, frustrates, and hinders the healing and restoration processes for survivors. We can do so much better. Of course, our country has always had communities facing compounding traumatic stress, particularly in cases where neighborhoods experienced oppression, hatred, poverty, addictions, and violence on an ongoing basis. Thankfully, organizations like the Equal Justice Initiative that is helping the country come to terms and make amends to great wrongs we have caused or perpetuated, and Fearless Dialogues that is helping people recognize our mutual humanity and work for change. Now, the same communities that have experienced decades of heartache and destruction, as well as communities that have experienced far more privileged circumstances, all are facing additional cascading tragedies. These include multiple natural disasters within close proximity, or combinations of natural and human-caused disasters, or combinations of natural and technological disasters, or disasters in communities amid overwhelming rates of opioid addictions and suicide. We must all do our part to consider the ways we can sustain ourselves and our neighbors amid impacts of trauma and disaster, add good back into a troubled world each day, and share strength and nourishment we have to offer to others as we go. Beyond our blogs, some of the ways that donors, volunteers, and staff at ICTG are making a difference is by providing a range of support for leaders. Leaders often need and want:
Please do not hesitate to reach out if you think any of these resources may be helpful to you. If you would like to encourage this critical work, I invite you to make a financial contribution today. Your generosity makes a great difference! Thank you.
|
�
COMMUNITY BLOGFrom 2012-2021, this blog space explored expanding understanding and best practices for leadership and whole-community care.
This website serves as a historical mark of work the Institute conducted prior to 2022. This website is no longer updated. Archives
January 2021
Categories
All
|


 RSS Feed
RSS Feed
